When managing Ebola virus disease (EVD), time is the ultimate variable. With an incubation period spanning 2 to 21 days, the virus begins with deceptively common symptoms—sudden weakness, muscle pain, and a sore throat—before rapidly escalating to severe gastrointestinal distress, organ impairment, and internal hemorrhaging. Carrying an average case fatality rate of 50% that can scale up to 90% in unmitigated settings, the stakes for immediate containment could not be higher.
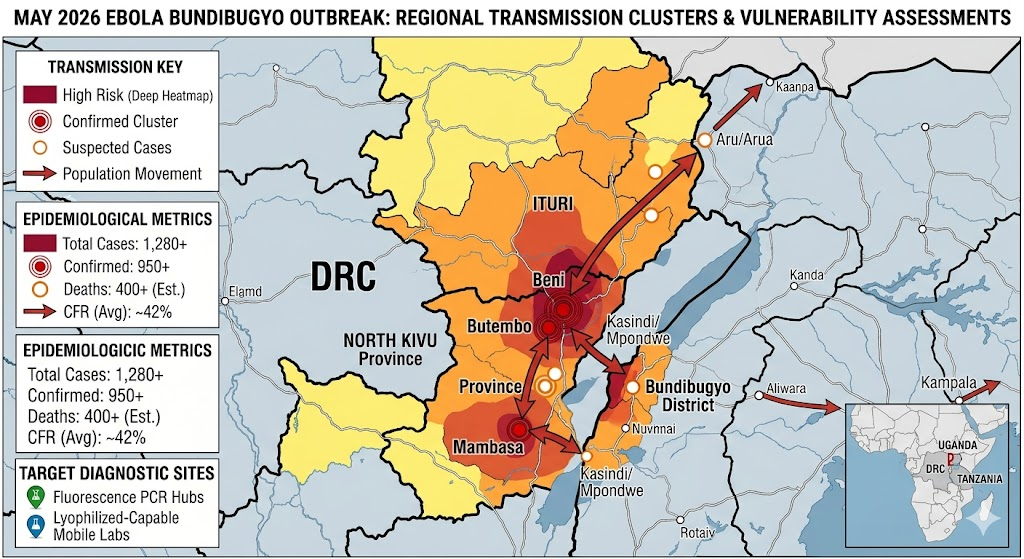
The true test for global health security is unfolding right now. The World Health Organization (WHO) recently declared the active multi-country Ebola outbreak a Public Health Emergency of International Concern (PHEIC). According to the latest joint monitoring data released by the WHO and the European Centre for Disease Prevention and Control (ECDC), the epidemic has rapidly evolved across central Africa, with the Democratic Republic of the Congo (DRC) Ministry of Health confirming active transmission clusters across Ituri, North Kivu, and South Kivu provinces, alongside cross-border cases in Uganda.
Crucially, this crisis is driven by the Bundibugyo virus variant (Orthoebolavirus bundibugyoense). As reported by Médecins Sans Frontières (MSF), this lineage presents an extraordinary threat because the revolutionary medical countermeasures developed after past epidemics—including approved vaccines like Ervebo and specific monoclonal antibody therapies—were engineered exclusively to target the Zaire ebolavirus strain. They offer no protection against Bundibugyo. Compounded by high population mobility along regional mining transit corridors and ongoing regional insecurity, preventing widespread geographic distribution depends entirely on rapid, definitive molecular screening to isolate cases before secondary transmission chains can form.
Because different Ebola variants dictate entirely separate clinical and containment strategies, vague symptomatic assumptions are dangerous. Frontline containment teams require advanced tools that can instantly differentiate genetic lineages without getting tripped up by co-circulating tropical threats like Marburg, Dengue, or Lassa fever.
The Power of Molecular Testing on the Front Lines
To eliminate this diagnostic blind spot, real-time Fluorescence PCR (Polymerase Chain Reaction) has become the gold standard for outbreak response. By targeting the genetic core of the virus rather than waiting for an antibody response, modern molecular engineering shifts how field clinics approach surveillance:
ulti-Strain Capabilities: Rather than limiting detection to one variant, sophisticated PCR assays utilize a multi-channel primer and probe architecture to identify a broad spectrum of lineages—including Bundibugyo, Sudan, Zaire, and Reston strains simultaneously.
Early Detection Limits: High-sensitivity molecular testing can achieve a minimum detection limit as low as 200 copies/mL, catching infections at the earliest stages when viral loads are low and symptoms are easily mistaken for less severe illnesses.
Flexible Specimen Sampling: In mobile field environments or border checkpoints, standard blood draws aren’t always practical or safe. Modern PCR protocols are fully validated for diverse sample types, including whole blood, serum, plasma, saliva, oral swabs, and urine.
Cold-Chain Independence: Recognizing that remote outbreak zones lack deep-freeze logistics, diagnostic platforms have adapted. Assays are increasingly available in lyophilized (freeze-dried) formats that remain stable at room temperature (2°C to 30°C), removing complex transport barriers.
Diagnostic errors can derail an entire containment effort. To prevent false negatives from sample degradation, advanced assays integrate a dual-channel design. The target virus is tracked on one specific fluorescence channel (such as FAM), while an internal amplification control (IC) runs concurrently via a secondary channel (such as VIC/HEX) to confirm the test executed perfectly. Furthermore, rigorous validation ensures zero cross-reactivity with look-alike pathogens like Marburg, Lassa, Yellow fever, Dengue, and Chikungunya.
These tests are engineered to be highly adaptable, running seamlessly on open-system real-time PCR platforms widely used across the industry.
Need reliable Ebola virus detection?
Explore our molecular diagnostic solutions designed for rapid, sensitive detection of multiple Ebola virus.